Vascular Risk Factors
 Smoking Smoking
High Cholesterol
Diabetes
Pregnancy and Hypertension
Male Sexual Dysfunction
|
Causes of Hypertension: |
|
 This is a question often asked, and the reply is often unsatisfactory. In the majority of patients, the cause is "benign essential hypertension -BET", a misnomer term because the effects over time may not be that benign. BET is usually hereditary and may have a genetic cause. A clue is that other family members may also have it. This is a question often asked, and the reply is often unsatisfactory. In the majority of patients, the cause is "benign essential hypertension -BET", a misnomer term because the effects over time may not be that benign. BET is usually hereditary and may have a genetic cause. A clue is that other family members may also have it.
Lifestyle causes are common, especially smoking. It may be the cause of the elevation in blood pressure, or maybe aggravating it. In either case no significant inroad will be made in treatment until you stop smoking.

|
|
Obesity is another major cause. For some people simple weight reduction may be a cure for their elevated blood pressure. Alcohol excess should be tackled. Bear in mind you do not need to be an alcoholic to have alcohol related blood pressure effects. Of course if your weekly consumption is too high then your blood pressure will rise. However if your weekly consumption is not that high, but it all comes at once (i.e. binges), then that can have equal effects.
Our main concern is that in a significant proportion of young patients (i.e. < 50 years), hypertension may be secondary to an underlying cause. This is important, as treatment of the underlying cause is essential. Conditions that can cause hypertension that may need to be excluded include other medication, previous kidney disease, over production of various hormones such as adrenaline (phaeochromocytoma), aldosterone (Conn's disease), and cortisol (Cushings syndrome ).
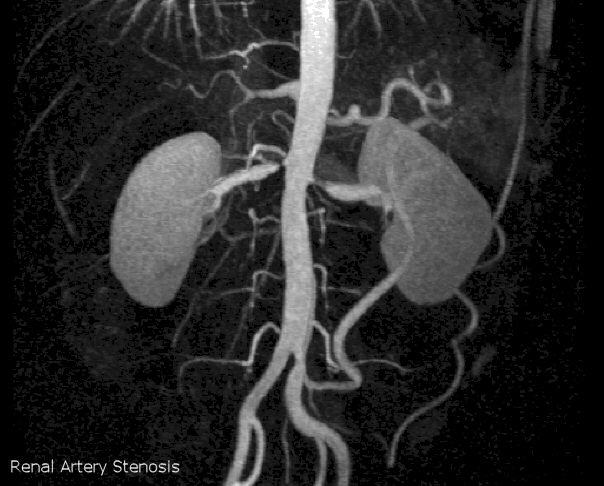
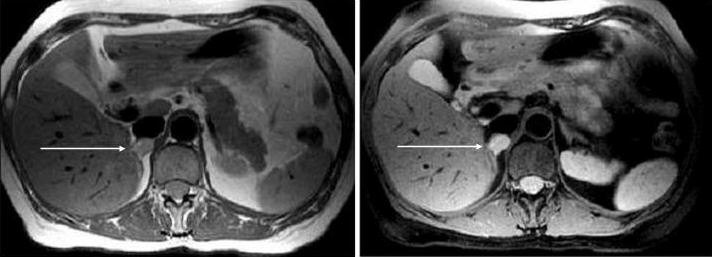
These conditions can usually be excluded by a series of blood tests, 24 hour urine collections, and scans. Before any consideration of fancy tests, the basic investigations include a full blood count to check for anaemia, blood salts (electrolytes), a chest X -ray and an ECG. More recently, cardiac magnetic resonance imaging has been used to exclude most causes of secondary hypertension such as coarctation of the aorta, renal artery stenosis and adrenal tumours (see below).



Making the Diagnosis
The diagnosis of hypertension, usually involves making 3 readings of blood pressure on separate occasions, performed by the family doctor or nurse using the conventional cuff. There are new guidelines on the threshold of blood pressure levels that require treatment. More recently, attention has focused on other special treatment groups or other vascular risk causes that need to be "factored in", when deciding at what threshold to treat the patient. (See figure 1.) Certainly in the presence of diabetes, peripheral vascular disease, previous stroke, or kidney disease, we would use a lower threshold of treating hypertension. The presence of target organ damage such as: protein in the urine, abnormal heart muscle thickening, and retinal eye blood vessel abnormalities would lower the threshold for treatment.
Blood pressure is a dynamic entity, fluctuating from day to day. In addition, blood pressure increases with age which can be a problem. The days are over when an elevation in blood pressure was ascribed to: "It's your age dear!" and not treated. Whilst it is your age (possibly!), all it means is we will be more aggressive about treating more elderly people as it is the blood pressure level and perceived cardiovascular risk level that dictates treatment.
Fluctuating Blood Pressure (or Labile Blood Pressure)
A lot of effort is spent deciding whether someone is hypertensive when the blood pressure readings are fluctuating. Of course if there are external forces around that time (e.g. worry about jobs, sick relatives, etc.) it may prudent to defer any further measurements until normality is restored.
However, if still an issue, the use of 24 hour ambulatory blood pressure (ABPM) or home monitoring as recommended by your family doctor may be helpful in determining the blood pressure status. If there are still issues then a referral to a specialist may help resolve the issue. When I am faced with such cases I examine the patient for the effects of blood pressure by assessing the target organs. This would provide clues that there has been an elevation in blood pressure that has affected target organs.
I check the eyes for thickened blood vessels, feel the pulses, check the heart for muscle thickening using EGGs and cardiac ultrasound, and checking kidney function with blood tests. By the end of this even the most elusive case can be diagnosed.
 What else can an elevation in blood pressure be due to? What else can an elevation in blood pressure be due to?
You guessed it, STRESS. Remember, blood pressure fluctuates throughout the 24 hour period, being lowest at night (unless you are a shift worker). Please also refer to the stress chapter.
In evolutionary times we became equipped with a series of protective reflexes (the autonomic nervous system) enabling us to deal with threatening situations; the flight, fight or fright scenario.This nervous system allows us to adjust our heart rate, blood pressure, etc so we could run away from such things as dinosaurs. These days for most of us, dinosaurs have been replaced by stress.
People do not necessarily own up to being stressed, or be aware of it. Certainly one does not want to fob off someone as being stressed; but at least explore the possibility.
There are other causes of elevations in blood pressure such as recreational substances and medication prescribed for other conditions (see table). If you think a medication is implicated, please consult your local doctor first.
Finally, an increasingly apparent cause is "White Coat Hypertension". The term is a misnomer as few of us wear white coats any more. There are two types: the one where you have no underlying hypertension, and the one where you are hypertensive (see later under treatment). In the former where although there is no underlying hypertension, the blood pressure goes up when someone measures it. There is no particular reason for this, but happens a lot. It can as likely happen as when a hospital doctor, family doctor or a nurse measures it.
What to do about it? As you would expect, the first thing is to get someone else to measure it. Otherwise, what we recommend you do is discuss this with your family doctor to have a 24 hour blood pressure monitor. The other alternative is to access a home blood pressure monitor either via the family doctor or a relative or friend who has one. Don't buy one at this stage unless the diagnosis is made.
Investigations:
These include the types of test to diagnose hypertension, those that assess the risk and prognosis of hypertension, and those that determine any underlying secondary cause.
|
|
|
|
|
|